Autonomic Nervous System Tutorial
Autonomic States
We are unaware of the subconscious control the autonomic nervous system (ANS) has over our everyday activities. Our pupils automatically respond to the amount of light, our hearts beat as required at the moment, we breathe even in our sleep...all of this without our conscious involvement. It's all controlled by a pair of neural divisions that quietly 'nudge our organs' in opposing directions. In essence, these two divisions maintain our organs in a 'middle ground' of autonomic tone, ready to either speed up or slow down, as local conditions demand.
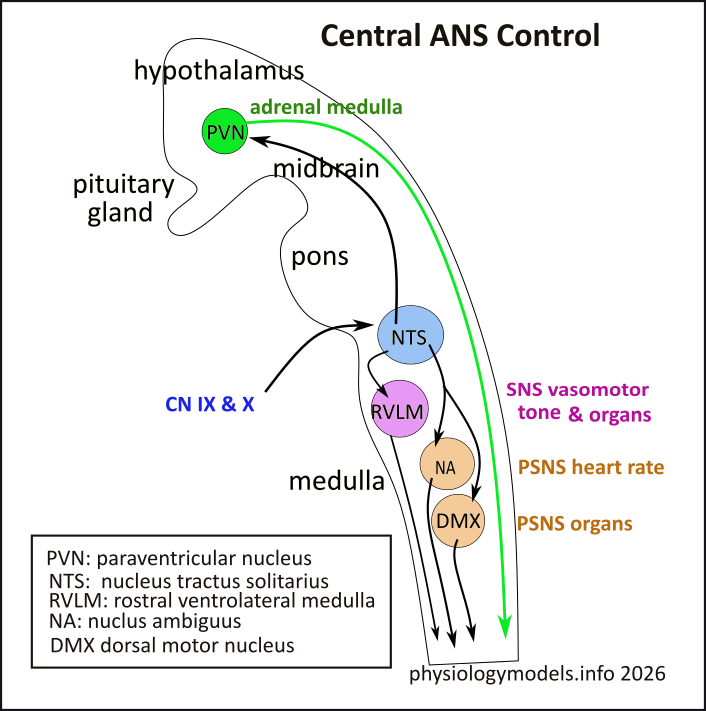
Though not usually considered in ANS tutorials, this illustration gives an overview of the centers in the brain that initiate the downstream neural signals of the sympathetic (SNS) and parasympathetic (PSNS) divisions of the ANS. I include this here simply to give the student a 'glimpse' of where it all starts.
The outline is a lateral view of the hypothalamus, midbrain, pons and medulla of the brain; it serves as a landscape for the locations of nerve centers (nuclei)...all are paired but only one of each shown. Most are clustered in the medulla; the arrows indicate where the nerve signals are go.
The NTS (blue) is the sensory-input center. Sensory receptors...stretch, chemical, blood pressure, etc...send information via cranial nerves (CN) IX (glossopharyngeal) and X (vagus) to this center. This information is analyzed and forwarded to the RVLM that sends signals down the spinal cord. There, they will synapse with SNS neurons leading to the arterioles, and other organs, that need 'adjusting'.
Sensory input from the heart, lungs and visceral organs is forwarded from the NTS to the NA or DMX...depending on the origin of the sensory input. Output from these nuclei lead to relevant PSNS neurons that are 'adjusted'.
Higher in the brain, in the hypothalamus, the PVN responds to stressful physical and emotional events by bypassing the medullary nuclei (green arrow) heading toward the adrenal medulla. Here, epinephrine (adrenaline) will be secreted into the bloodstream causing a diversion of blood to 'vital' organs; the result is the 'fight-or-flight' response that characterizes stress and is often associated with SNS responses.
Again, the above is a prelude to the autonomic nervous system. If you are a student, it is unlikely you will be held responsible for the information presented there.
***************************
A Picture is Worth...
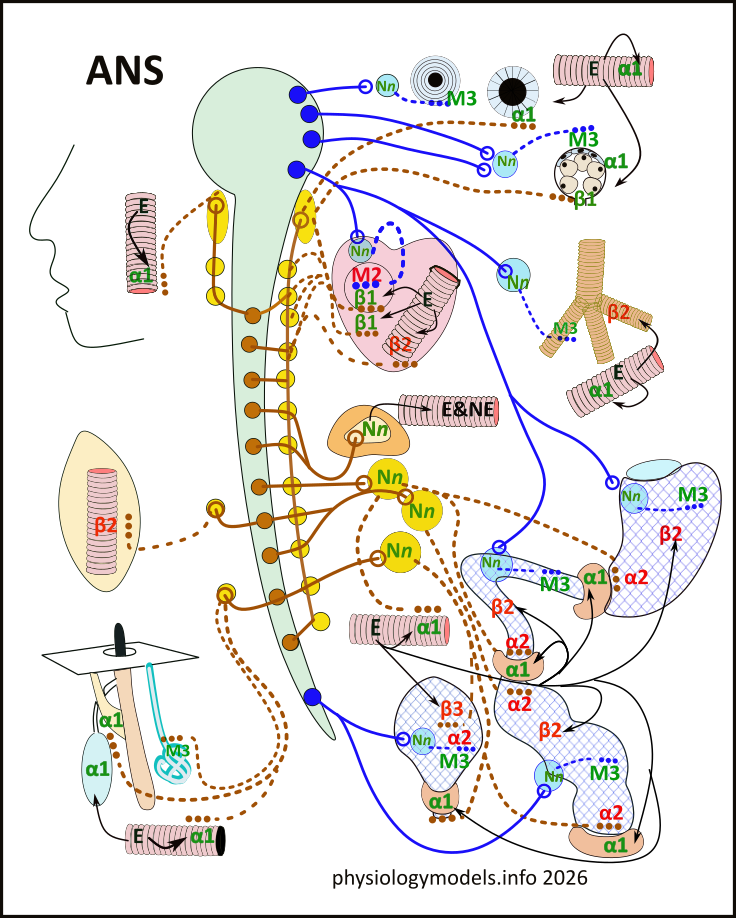
This model offers a visual, compressed, symbolic representation of the neural pathways and organ responses to the two divisions of the autonomic nervous system (ANS). One division, the parasympathetic (PSNS) division, exits the central nervous system (CNS) from the brain and sacral spinal cord. It is called the craniosacral outflow. The other division, the sympathetic (SNS) division, exits the CNS from the thoracic and lumbar regions of the cord. It is called the thoracolumbar outflow.
Color-coding plays an important role. For instance, the PSNS neurons (nerve cells) are blue while the SNS neurons are brown. If the receptors for neurotransmitters stimulate the organ they are color-coded green; if the receptors inhibit the organ they are color-coded red.
The first portion of this tutorial explains the anatomical layout (pathways) of the neurons in each division. Details about the inclusion of these neurons within spinal nerves and the formation of ganglia (lumps along a nerve) are described. This is followed by descriptions of the neurotransmitters and their receptors. This first section ends with how the regulation of blood flow to specific organs amplifies the normal activities of the SNS.
The following portion of this tutorial describes, in detail, the interplay of the two divisions within selected organs. There is little description of the biochemistry involved in local control of these organs...that is the purview of other tutorials within this website. A final section, ...A Thousand Words, summarizes the information that has been presented in a visual format.
Cephalic Structures
The large open circle with a long hollow tail running the length of the model represents the brain and spinal cord. All nerves exit on both the right and left sides...only one side is illustrated.
The outline of a face shows a blood vessel that supplies the oral and nasal linings (mucosae). To the right of the brain are two images of the iris of the eye; one with the pupil constricted and the other with the pupil dilated. Below these is a round structure that represents one of three pairs of salivary glands.
Parietal Structures
Below the face is the blood supply of a skeletal muscle and below that is a section from the skin. This shows a hair follicle and two sweat glands. The 'E' within the blood vessels represents the hormone epinephrine (adrenaline).
Visceral Structures
The heart and lungs are in the thoracic cavity; only the bronchial tree is illustrated showing circular muscles around the bronchioles. The heart shows its pacemaker (circle) and cardiac blood vessels within the myocardium (cardiac muscle).
The abdominal cavity shows the adrenal gland, the stomach and intestines, and the urinary bladder. The three donut-shaped structures are sphincters.The three large yellow circles are the collateral ganglia.
***************************
ANS Neural Pathways
The small, solid-colored circles that have solid or dashed lines extending from them represent individual neurons cell bodies. Their axons travel within large nerves of the somatomotor nervous system (not shown). Pathways from the CNS, to the organs, consist of two neurons in a row. The model only shows single neurons but there are actually hundreds lying side by side within a nerve.
The first neuron's cell body (circle) is within the brain or spinal cord (CNS). It's axon (solid line) leaves the CNS, travels within the large nerves, and synapses with the cell body (circle) of the second neuron. Since there are numerous parallel neurons within a nerve, the cell bodies of the second neurons forms a visible lump along the nerve. This lump is a ganglion. The axon of the second neuron (dashed line) leaves the ganglion to innervate organs within the body. The first neuron is referred to as preganglionic ('pre') while the second is postganglionic ('post').
The ANS consists of two divisions: parasympathetic (PSNS) and sympathetic (SNS).
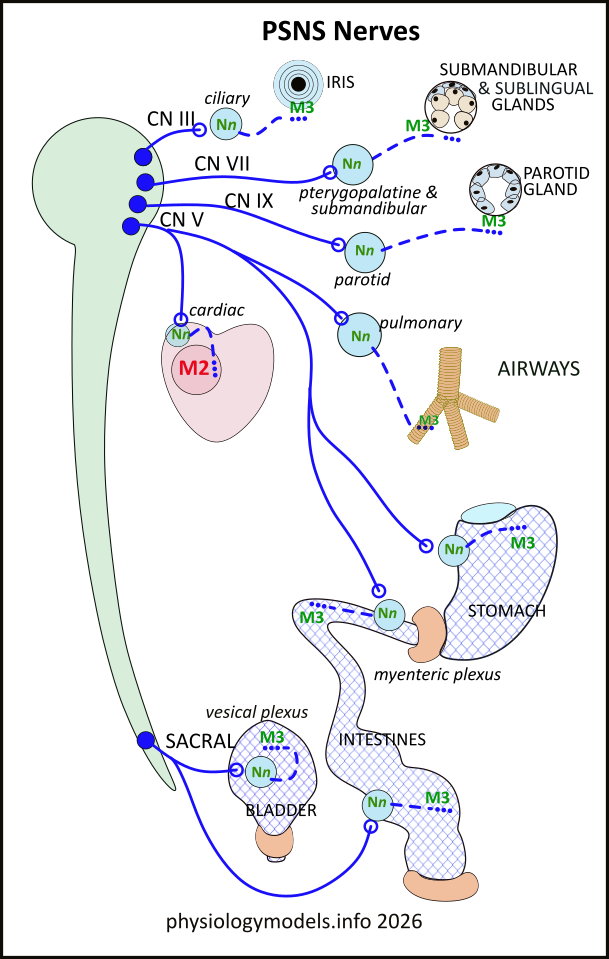
Parasympathetic Pathways
This is the 'rest and digest' division of the ANS. When its activities are stronger than those of the SNS the pupils are small, the oral and nasal linings (mucosae) are moist, salivary glands are active, airways are maintained for efficient air flow, the heart rate is slow, digestive and excretory systems are functioning. These are the hallmarks of PSNS activity...resting and digesting.
This 'take out' from the model isolates the anatomical arrangement of the PSNS division. Several generalizations are apparent:
***************************
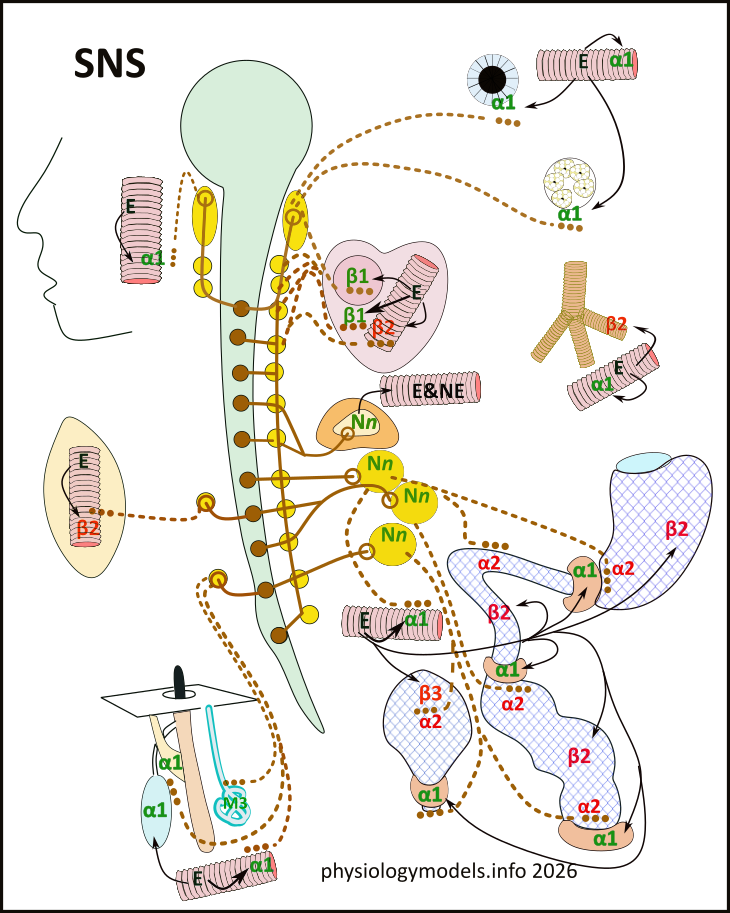
SNS Pathways
This is the 'fight-or-flight' division of the ANS. In addition to innervating the same organs as the PSNS, it innervates blood vessels throughout the body and organs located in the parietal region. When SNS activities are stronger than those of the PSNS the pupils are dilated, the mouth is dry (like cotton), the skin is pale (white with fright) and clammy, the heart races and pounds, hair 'stands on end', blood flow to 'non-vital' organs is reduced and redirected to the 'vital' skeletal muscles and heart...fight or flight.
This 'take out' from the model isolates the anatomical arrangement of the SNS division. It is much more complex than the PSNS yet generalizations can still be made:
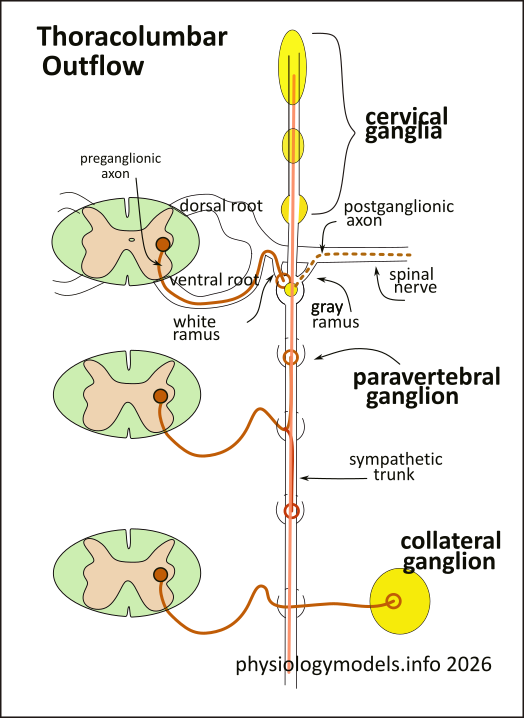
Thoracolumbar Outflow
The abundance of ganglia complicates understanding the SNS pathways. This illustration details how the somatomotor neurons of the spinal nerves and SNS neurons are combined.
The most obvious structure is the vertical chain of paravertebral ganglia. There are a pair of them...only one is drawn...side by side against the ventral surface of the bony vertebral column (not shown). The cross-sections of the spinal cord indicate the area of gray matter that contains the SNS preganglionic cell bodies (brown circles).
Spinal nerves (outlined) exit through a foramina (small opening) between each vertebra; they exit as a pair of 'roots'...dorsal and ventral. These roots fuse, forming the nerve, just as it becomes visible between the bones.
The spinal nerves contain sensory neurons entering the cord via the dorsal root and motor nerves leaving via the ventral root. It is from the ventral root that a short branch (white ramus) leaves the nerve and enters a paravertebral ganglion within the chain. This ganglion houses cell bodies (yellow circle) of the postganglionic neurons whose axons (dashed lines) reenter the spinal nerve via the gray ramus.
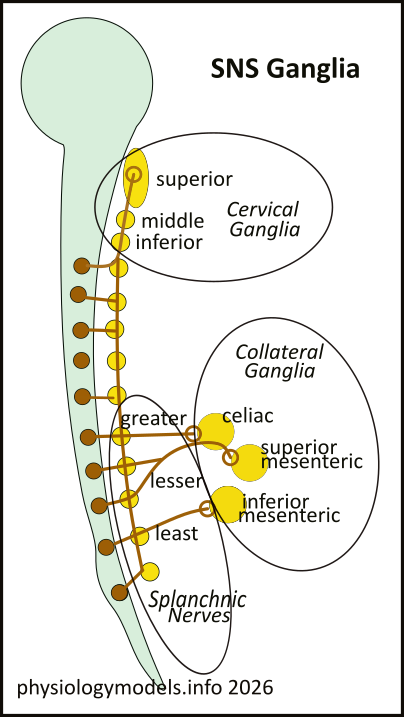
SNS Ganglia
Superimposed on what was just described are additional 'pre' axons that branch and turn up and down the chain to connect with nearby ganglia. This happens throughout the chain of ganglia forming a sympathetic trunk that unites them.
Beside the cervical cord...where no 'pre' axons exit...there are three ganglia pairs of 'post' cell bodies. These are the superior, middle, and inferior cervical ganglia. A glance back at the model shows their 'post' axons innervating the eye, salivary glands, heart and mucosae.
Postganglionic axons, from T5-L2, combine and form a plexus (branching network of intersecting nerves) surrounding the midline celiac artery, extending from the aorta, just behind the stomach. These are the splanchnic nerves: greater, lesser, and least. They innervate the unpaired collateral ganglia: celiac, superior mesenteric, and inferior mesenteric that house the 'post' cell bodies.
***************************
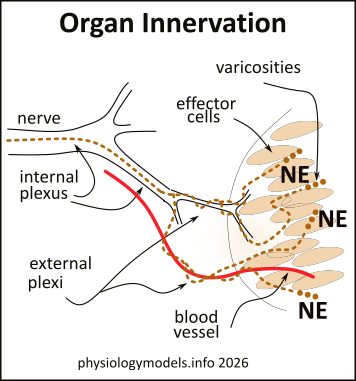
Varicosities
Varicosities are bead-like swellings along and at the end of 'post' axons. They store neurotransmitters that, when released, bathe the surrounding cells. The illustrations only show the last three.
The innervation of 'post' axons in both divisions is the same. On entering the organ, the axons release their neurotransmitter throughout the tissue of the organ, much like a soaker hose. All the cells are bathed, but the neurotransmitter only attaches to specific receptors (see chart below); others are ignored. Since both divisions are autonomically active, both PSNS and SNS neurotransmitters diffuse throughout the tissue at the same time...though in different concentrations depending on local controls within the organs (not specifically described in this tutorial).
Though illustrated as individual neurons, there are actually many, side by side, within the nerves. The 'pre' may branch up to 10 times traveling toward the 'post' cell bodies in ganglia. The 'post' axons also branch, and branch even more, after entering the organ they innervate.
Though this illustration shows only one axon, after branching, an internal plexus of them travels within a nerve. On nearing the organ, the axons move to the surface of the nerve, or along small blood vessels. After penetrating the organ, they branch numerous times spreading throughout the tissue. These branches form hundreds of varicosities that release their neurotransmitter into the interstitial fluid bathing the organ's cells.
***************************
Neurotransmitters
Effectors are the cells that display receptors for specific neurotransmitters; they are the cells in the organ that cause (effect) a response. Smooth muscle cells and cardiocytes contract, glands secrete, pacemakers change their rate of firing, and neurons send impulses. But, an 'effect' can be either positive (stimulatory) or negative (inhibitory). In the model, receptors that cause a stimulatory response are color-coded green while those that cause an inhibitory response are color-coded red.
Neurotransmitters are the chemicals stored at the end of the 'pre' and 'post' axons. Boutons (buttons) are found at the end of 'pre' axons while and varicosities are at the end of 'post' axons. The boutons are illustrated as small circles at the end of 'post' axons; varicosities are represented as three small dots.
To manage day-to-day autonomic tone and local adjustments, the CNS relies on a hierarchy of centers in the brainstem and hypothalamus. These act as the "integrators" that receive sensory feedback and adjust the output of the sympathetic and parasympathetic divisions.
Receptors
On receiving signals from the CNS, the innervated 'pre' cell bodies release their neurotransmitter molecules that end in a ganglion. This stimulates the 'post' cell bodies, that form the ganglia, to release their neurotransmitter within the organs they innervate. What happens depends on the receptor that is displayed on the tissue cells of the organ. These cells are called effectors because their response IS the effect caused by the neurotransmitter.
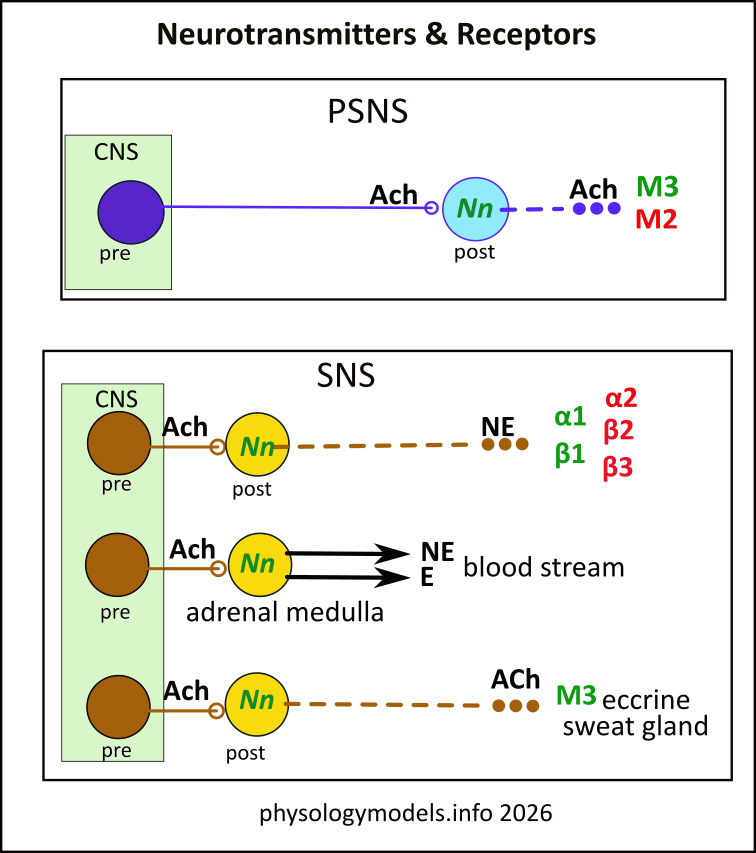
This chart summarizes the neurotransmitters of 'pre' and 'post' axons of both divisions and the receptors they combine with. In the PSNS and SNS there are boutons at the end of 'pre' axons that release acetylcholine (ACh) onto Nn receptors on 'post' cell bodies within ganglia. These stimulated (green) neurons will release their neurotransmitter molecules on effector cells within the organ they innervate.
The top box in this illustration shows that the 'post' of the PSNS also releases Ach. The receptors ACh can combine with are muscarinic; M3 cause stimulation (green) of the effector cells that display them while effectors displaying M2 will be inhibited (red).
The lower box in the illustration shows three pathways by which the SNS causes its effects. The most common way is the top picture: the 'post' cell bodies contain Nn and ACh stimulates them to send release their neurotransmitter in the organ they innervate. The neurotransmitter released is norepinephrine (NE) and there are 5 possible receptors for it. Attachment of NE to alpha1 or beta1 receptors will stimulate (green) the effector cell; alpha2, beta2 and beta3 all inhibit (red) their effector cells.
The last two pictures show the 'exceptions to the rule' of SNS releasing NE from 'post' varicosities. The middle picture shows what appears to be a 'post' cell body without an axon. This is actually the case for the adrenal medulla. When its cell body Nn receptors are activated they release norepinephrine (NE) and epinephrine (E) directly into the bloodstream. This will be described in detail later in the tutorial.
The last picture shows the 'post' axon releasing ACh, instead of NE, on a M3 receptor. This is the situation in eccrine sweat glands which, also, will be described below.
***************************
Blood Flow
An arteriole is a branch off an artery that leads to a capillary bed within an organ. Their walls are mainly circular layers of smooth muscle. They are narrow, with a SNS vasomotor tone that maintains their diameters within a fraction of a millimeter.
Upon this autonomic background, the metabolic activities of the organs they supply also have local control. Normally, active tissues utilize oxygen and secrete carbon dioxide into the surrounding interstitial fluid. These compounds diffuse to sphincter muscles located at the start of capillary beds where the incoming arteriolar blood enters. Low oxygen and high carbon dioxide cause the circular smooth muscles in these sphincters to relax and increase capillary flow. In inactive tissues the conditions are reversed and the sphincters are more contracted reducing flow through the capillaries.
Stressful conditions result in an override of this autonomic tone and blood distribution. The 'fight-or-flight' responses associated with the SNS require a diversion of blood flow away from 'non-vital' organs and a increased flow to 'vital organs'...the heart and skeletal muscles. The model shows arterioles that lead to selected capillary beds that best demonstrate the effects of vascular epinephrine (E).
The circular arrangement of smooth muscle cells forming the walls of an arteriole is ideal for changing its diameter. If stimulated, their constriction narrows the vessel. They do not have any inhibitory PSNS signal to relax...the pressure of the flow of blood keeps them open. The major difference in E receptors that determine where blood flows is that those leading to the heart and skeletal muscles have inhibitory (red) beta2 receptors while those elsewhere have stimulatory (green) alpha1 receptors. It is these differences that produce the extreme effects that occur when stressed.
Under stressful situations, strong stimulation of the adrenal medulla causes the release of 20% NE and 80% E. The more abundant and more potent of the two is shown in arterioles throughout the model. Arrows indicate it alters the diameter of the arterioles it flow through but also diffuses from capillaries throughout the body. Arterioles that display alpha1 (green) receptors constrict, reducing blood flow through them. Those that display beta2 (red) relax, increasing blood flow through them.
The arterioles that display beta2 receptors supply the heart and skeletal muscles that are 'vital' to survival. The rest are considered 'non-vital' and display alpha1 receptors. This arrangement diverts blood flow from 'non-vital to 'vital' organs to enable the 'fight-or-flight' responses characteristic of the SNS division.
This ends the foundational information that describes the ANS. The following sections of this tutorial describe details about specific neural pathways and reactions.
***************************
Adrenal Medulla
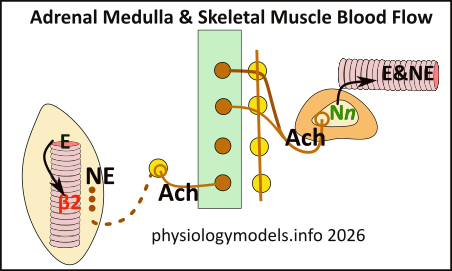
Normally, there is no output from the adrenal medulla. It becomes active when centers within the hypothalamus of the brain, integrating sensory and emotional input, determine the necessity of a systemic...full body...response to stressful situations. If needed, descending signals are sent down the spinal cord directly to the 'pre' cell bodies leading to the adrenal gland. The release of E into the bloodstream provides a systemic pathway to all the organs.
Inspection of the model shows the adrenal medulla only has SNS innervation. Several 'pre' axons from the thoracic cord pass through the paravertebral ganglia of the two chains without stopping. They mix with the neurons of the celiac plexus (solar plexus) and penetrate the adrenal glands.
They pass through the cortex of the gland and continue into the central medulla. There they synapse with chromaffin cells that bear Nn receptors. These cells can be considered modified 'post' neurons that lack axons. The medullary effectors respond by releasing 80% epinephrine (E) and 20% norepinephrine (NE) directly into the bloodstream.
These two neurohormones diffuse from capillary beds throughout the body; of the two, E is the more potent. Its differential effects on arterioles diverts blood flow from 'non-vital' organs to 'vital' ones. Flow is increased to the heart and skeletal muscles and reduced elsewhere.
This illustration shows what occurs in a skeletal muscle. Even though NE from day-to-day SNS innervation facilitates flow to the muscles, E from the bloodstream greatly amplifies the flow. The black arrow, pointing from E to the inhibitory (red) beta2 receptor of the arteiole wall, indicates that vasodilation will facilitate blood flow to these muscles.
***************************
Heart
There are two effector tissues in the heart; the nodal cells of the pacemaker and the cardiac muscle cells of the myocardium. The pacemaker, the sinoatrial node (SA), is in the wall of the right atrium where the superior vena cava enters. It is innervated by both the PSNS and the SNS.
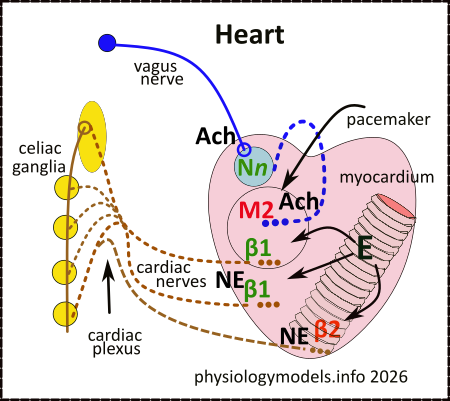
The PSNS pathway begins in the brain and long 'pre' axons travel within the vagus nerves directly into the heart itself. The cell bodies of 'post' neurons form an intramural ganglion (light blue circle) with Nn receptors for ACh. Short 'post' axons spread out in the SA node and release acetylcholine (ACh) from their varicosities. This inhibits (red) the muscarinic 2 (M2) receptors on the nodal cells and decreases the heart rate.
The 'post' axons of the SNS pathway originate in the three cervical ganglia and the first ganglia just below them. Their axons form the cardiac plexus and continue as cardiac nerves to both the pacemaker and the myocardium. Both regions have stimulatory (green) beta1 receptors on the effector tissue. The effects are to increase the heart rate and the forcefulness of the ventricular contractions when NE, from their varicosities, combines with them. Additionally, NE is released from SNS axons and dilates those arterioles.
Normally, the balance between both divisions establishes the heart rate and contractility. In stressful situations, the increased amount of powerful epinephrine (E), diffusing from capillaries, takes control and floods both the myocardium and dilates the arterioles. The heart 'races' and 'pounds'.
***************************
Dermis
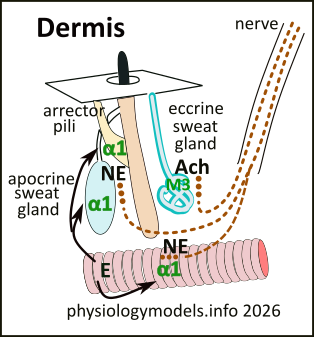
The dermis has apocrine and eccrine sweat glands and arrector pili smooth muscles that run from the lower surface of the epidermis to the side of hair follicles. Normally, these muscles aren't contracted, and hairs lie relatively flat on the skin. The apocrine sweat glands, found in the armpits and groin area, empty minimal secretions into hair follicles there.
The eccrine sweat glands, with ducts leading directly to the surface of the skin, are involved in thermoregulation. The hypothalamus senses changes in blood temperature. To reduce the temperature, it increases SNS ACh release onto eccrine glands to increase sweating. Simultaneously, it decreases the SNS signals to the 'constricting' alpha1 receptors on dermal blood vessels bring the warm blood to the surface. This combination facilitates sweat evaporation and heat loss. The opposite activities would conserve heat.
Under stressful situations, the vascular epinephrine (E) overrides normal vasomotor tone of dermal arterioles reducing blood flow to the extent that sweat production is reduced and the skin becomes clammy and pale..."white with fright". The E also stimulates alpha1 on apocrine sweat glands increasing "nervous sweat" and stimulates arrector pili muscles causing the hair to "stand on end".
***************************
Iris
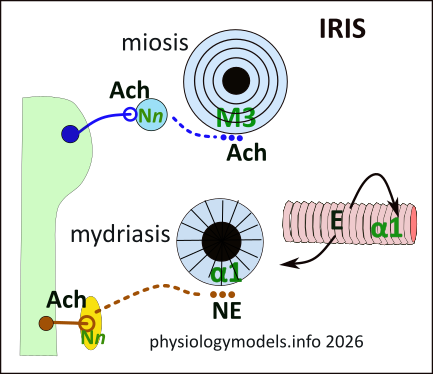
The iris of the eye has two intermingled sets of smooth muscles surrounding the pupil: circular and radial. The circular muscles are innervated by the PSNS and display stimulatory M3 receptors for the ACh released by the 'post' varicosities of the PSNS. The radial muscles, innervated by the SNS, display stimulatory alpha1 receptors for the NE released by the 'post' SNS varicosities.
Contraction of the circular muscles results in a smaller pupil...miosis. Contraction of the radial muscles causes the pupil to dilate...mydriasis. Normally the pupil size reflects the simultaneous activity of both divisions and the pupil size is somewhere between these two extremes.
Even though stressful situations reduce the blood flow to this region, the vascular epinephrine (E) is sufficient to stimulate the alpha1 receptors on the radial muscles causing the pupils to dilate.
***************************
Salivary Glands
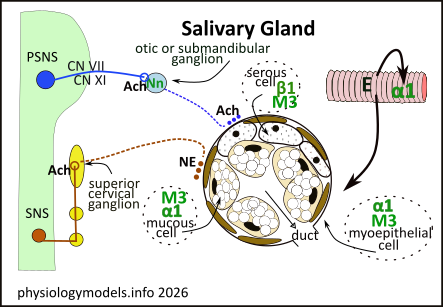
There are three pairs of salivary glands: parotid, submandibular, and sublingual. They can contain three types of cells: serous, mucous, and myoepithelial that are arranged in acini (grapes). These feed into a compound, branching tubular network leading into the mouth.
All acini are surrounded by a basement membrane that 'post' axons penetrate but remain on the surface of the acini instead of penetrating between the cells. The neurotransmitters they secrete diffuses over all the cells. This illustration shows each type. The outer layer of brown cells are stellate (star-shaped) myoepithelial cells that are contractile. The three freckled cells at the top of the acinus are serous cells. The central mucous cells show numerous white mucinogen droplets.
Parotid Glands
Approximately 25% of saliva is from the parotid glands. They contain serous cells that secrete water, salts and enzymes. The enzymes are produced in zymogenic granules (freckles) throughout the cytoplasm. Their duct, Stensen's duct, enters the mouth opposite the 2nd upper molar.
The PSNS 'pre' axon travels in CN IX (glossopharyngeal nerve). These release ACh within the otic ganglion that stimulates, via Nn activation, the release of ACh from the varicosities on the 'post' axons. The ACh diffuses over these cells stimulating the M3 receptors found on the serous and myoepithelial cells.
The SNS 'post' axons arrive from the superior cervical ganglion; their varicosities release NE at the acinar surface. This diffuses throughout the acini activating beta 1 receptors on the serous cells and alpha 1 receptors on the myoepithelial cells.
The SNS B1 receptors stimulate the release of enzymes from the zymogen granules of the serous cells. The PSNS M3 receptors cause the release of NaCl, into the acinar lumen, that causes water to follow by osmosis. This provides a medium to carry the enzymes from the gland. The SNS alpha 1 receptors on the myoepithelial cells 'squeeze' the acini to move the saliva down the duct system.
Submandibular Glands
The submandibular glands, located below the mandible, contains both serous and mucous cells, as in the illustration, and supply ~70% of the saliva through Wharton's duct in the floor of the mouth.
The PSNS 'pre' axons exit the brain within CN VII (facial nerve). They release ACh from their boutons within the submandibular ganglia. The 'post' axons, as with all other innervation to the acini, release their neurohormone (ACh) at the surface of the structure. The activation of M3 receptors cause NaCl and water to enter the lumen as described above.
The SNS 'pre' axons are from the superior cervical ganglion and release NE at the acinar surfaces. The alpha 1 receptors on the mucous cells cause the droplets to migrate to the surface and release their contents. The mucin rapidly hydrates, swelling to physically move the secretions through the duct system. Additionally, alpha 1 on the myoepithelial cells gives an added 'squeeze'.
The serous cells of these acini functions as mentioned above. The mucous cells produce such numerous and large mucinogen droplets that, in slides, the nuclei appear flattened against one side of the cell. There are small canaliculi (small canals) between the mucous cells to allow movement of the serous secretions into the lumen.
Sublingual Glands
The sublingual glands, located beneath the tongue, contain mostly mucous cells and open through numerous small openings (ducts of Rivinus). They secrete 5% of the total saliva.
The PSNS and SNS pathways are the same as those of submandibular glands. The responses of M3 and alpha1 receptors of the mucous cells are the same as described for the submandibular glands.
Normally, the activity of these glands depends on the composition of the food we are eating. Generally speaking, sour (acidic) and bland, dry foods stimulate PSNS activities. The major receptor, M3, activates the parotids to provide the 'watery environment' most beneficial for this intake. Starchy and fatty foods activate the SNS more to release enzymes from the serous cells (beta 1) and mucus from the mucous cells (alpha 1).
Stressful conditions again demonstrate the diversion of blood flow from 'non-vital' to 'vital' organs. The epinephrine (E), from the adrenal medulla, activates alpha 1 receptors on the salivary arterioles (non-vital). Their constriction reduces the water supply for saliva production leading to a 'dry mouth' sensation.
***************************
Airways
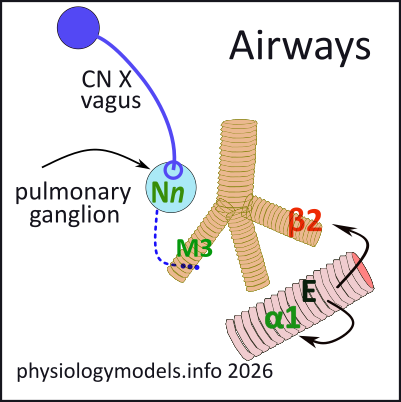
The bronchioles of the lungs don't have SNS innervation. The PSNS innervation is from CN X (vagus) that releases ACh on the pulmonary ganglia. From there, the 'post' axons varicosities release ACh on the circular smooth muscles of these airways. The bronchoconstriction this causes does not close the passages but maintains an autonomic tone for efficient air passage.
The effects of stress are seen when vascular epinephrine 'overrides' vasomotor tone. Even though the E causes vasoconstriction of the arterioles to this 'non-vital' organ, its potency is sufficient to cause bronchodilation, due to inhibitory (red) beta 2 receptors on the airways.
***************************
GI Tract
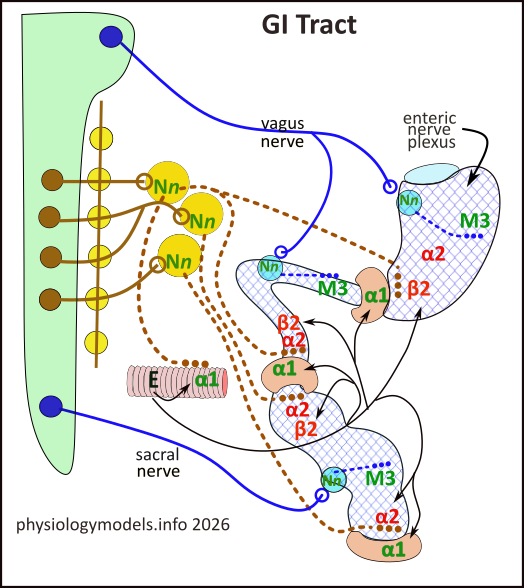
Only the stomach, small and large intestines are illustrated. The three tan donuts are circular-smooth muscle sphincters. The pyloric sphincter separates the stomach and small intestine, the ileocecal separates the small and large intestine, the internal anal sphincter is at the end of the anus.
The 'net' in the GI tract represents a massive nerve plexus (myenteric or Auerbach's plexus) between the circular and longitudinal smooth muscle layers. It is not part of the ANS but a separate intrinsic (internal) network unique to the GI tract. The release of ACh and NE activate receptors on this network (not described here) that amplify the effects of the ANS neurotransmitters.
The PSNS 'pre' cell bodies (dark blue circles) are within the brain and sacral cord; their axons travel within CN X (vagus nerve) and the sacral nerve. These long axons innervate their 'post' ganglia that are intramural. These axons branch numerous times displaying hundreds of varicosities that release ACh on stimulatory (green) M3 receptors displayed on the smooth muscle cells causing the peristaltic and segmental contractions of the gut.
The SNS 'pre' cell bodies (brown circles) are in the spinal cord and their axons pass through prevertebral ganglia of the 'chain' to innervate collateral ganglia (three large yellow circles). These 'pre' axons release ACh on the 'post' cell bodies in the collateral ganglia that display stimulatory (green) Nn receptors.
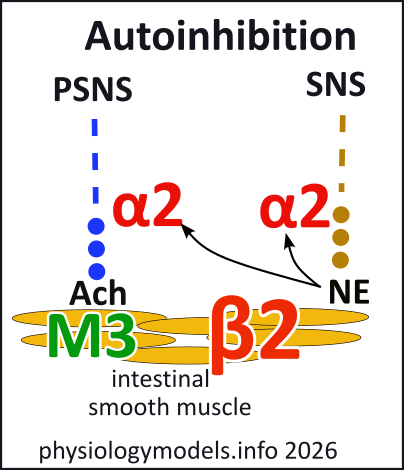
Stimulated SNS 'post' axons release NE on several receptors throughout the gut. (1) There are stimulatory (green) alpha 1 receptors on the sphincters causing them to constrict. (2)There are inhibitory (red) beta 2 receptors on the smooth muscles that inhibit their contractions. (3) There are inhibitory (red) alpha 2 receptors on the varicosities of both PSNS and SNS axons as shown the 'Autoinhibition' illustration.
This illustration shows the effects NE has on alpha 2 receptors displayed on SNS and PSNS varicosities. These receptors are on neurons; when NE binds to them they inhibit their neurotransmitter release. The PSNS secretion of ACh is reduced and the SNS secretion of NE is too. In other words, active SNS activity is self-limiting.
As usual, during stressful situations, the 'override' of E...note black arrows in previous illustration...reduces blood flow to this 'non-vital' organ and essentially closes it down. Notice all the beta2 receptors that are affected by E!
***************************
Urinary Bladder
The detrusor muscle of the urinary bladder has smooth muscle cells arranged at many angles resulting in a 3D squeeze to eliminate urine. Its orifice is surrounded by an internal and external sphincter. The internal is under ANS control while the external is under conscious control.
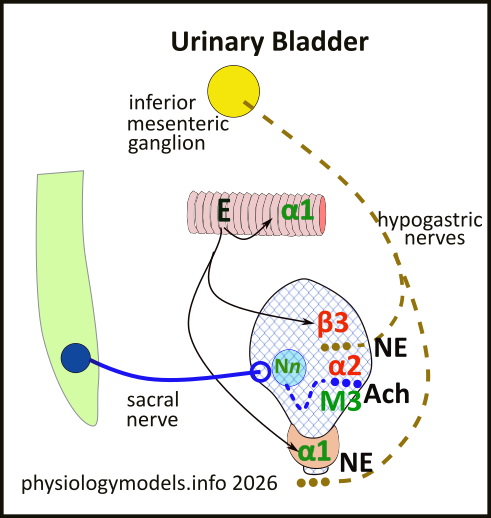
The PSNS innervation begins at the sacral cord with the 'pre' axons, traveling within the sacral nerve, innervating intramural 'post' ganglions. The release of ACh from their varicosities binds with stimulatory (green) M3 receptors that cause contraction of the detrusor muscle. This 'inappropriate' response is not characteristic of the 'rest-and-digest' scenario.
There are two mechanisms that prevent this embarrassing situation. A center in the brainstem establishes an 'autonomic tone' that suppresses the activation of the downstream sacral 'pre' cell bodies leading to the bladder. In case this doesn't 'do the trick', the NE from SNS 'post' varicosities binds with inhibitory (red) alpha 2 receptors on the PSNS varicosities...similar to what occurs in the GI tract. This directly inhibits any ACh that might be released.
The SNS 'post', from the inferior mesenteric ganglion, releases NE that keeps the PSNS inhibited...as just described... and, binding to inhibitory (red) receptors, suppresses muscle contractions. Norepinephrine also binds with stimulatory (green) alpha 1 receptors on the internal sphincter keeping it closed. At this point, one might wonder, "How is urine voided"?
Stretch receptors in the bladder wall, at a 'critical' point, send afferent signals to the CNS that removes the the brainstem suppression signal allowing activation of the sacral PSNS pathway to the bladder. Simultaneously, brainstem signals also inhibit SNS outflow from the cord that leads to the inferior mesenteric ganglion. This stops the release of NE in the bladder wall thus removing the 'local' inhibition of ACh release from PSNS varicosities. The tonic constriction of the internal sphincter is also gone. Conscious relaxation of the external sphincter enables voiding.
Under stressful situations, vascular E reduces blood flow to this 'non-vital' organ. However, the beta 3 receptors of the detrusor muscle keep it relaxed. Plus, the internal sphincter contraction is reinforced.
***************************
...A Thousand Words
It is amazing to realize that our organs are subconsciously held 'in the ready' to respond appropriately to whatever situation might occur. This so called 'autonomic tone' resembles driving a car with one foot on the accelerator and the other on the brake. For example, the heart's pacemaker normally beats neither too fast (accelerator) nor too slow (brake). It is 'held' in this mid-zone (autonomic tone) because it is simultaneously receiving neural signals from the SNS to 'speed up' and also signals from the PSNS to 'slow down'.
But it's not the signals themselves that cause these responses but rather the receptors on the surface of the pacemaker cells. There are two of them: one that, on being signaled, increases the heart rate, and the other that decreases it...stimulatory and inhibitory receptors. The pacemaker continuously receives both signals, but in different concentrations. This 'middle ground', between fast and slow, is the 'autonomic tone' of daily life. The average adult heart rate is between 60 to 100 beats per minute.
But organs are large; how can only a nerve or two supply enough neurotransmitter molecules to each effector cell simultaneously? The 'pre' neurons may branch 10 to 20 times as they travel toward their ganglia. The 'post' neurons branch many more times while traveling toward the organ. And, on entering the organ, their axons branch many more times while diving deep between the effector cells. And, each branch has hundreds of neurotransmitter-filled varicosities. Upon released the neurotransmitter molecules diffuse throughout the tissue, initiating a coordinated response across the organ within seconds.
There are local controls within each of our organ systems that send neural 'feedback' to the brain as to whether or not its 'tone' is sufficient for the specific task at hand. Several are mentioned in the tutorial, but not all. Suffice it to say that, on receiving this feedback, the central ANS control (see introduction) responds by altering the strengths of the SNS and PSNS signals being sent to the 'complaining' organ. As a result, the activities of the organ either increase or decrease in response to its current situation.
This is how we survive, day to day, until our brain responds to 'stress'. Stress is anything that causes the well recognized 'fight-or-flight' scenario. This total-body response is due to the 'adrenaline rush' all have felt at one time or another. Its because adrenaline (epinephrine) has suddenly been released into the bloodstream from the adrenal medulla glands. It diffuses from capillaries throughout all the body after first diverting blood from 'non-vital' organs to the heart and skeletal muscles...the 'vital organs'. 'Robbed' of sufficient blood flow, the activities of 'non-vital' organs are significantly reduced.
Unfortunately, a summary of the ANS leads to lists you might feel compelled to memorized. However, I have found that the mind can retain a picture much longer than it can keep any list straight. But this does not negate the requirement that hours must first be spent to understand what the picture represents.